


Wikipedia is a good beginning for this prompt question, which specifically asks for a description of ‘my’ morning rituals’. Ritual is, in my selective understanding at least, primarily a social phenomenon that enacts a prescribed means, sometimes to the minutest detail, of expressing the invisible and numinous in a process. It manifests the ways in which a person or group enters into a communion with the unseen and possibly otherwise incomprehensible, which for our age includes the puzzle of the nedd to come to terms with complex identity configurations in time and space.
However, it seems proper to excerpt,at least, from Wikipedia’s opening descriptions and discussion of the word’s etymology for the word ‘ritual’ to raise the issues I think we need to clarify first. These are reducible thus: how, if rituals are, as I believe, primarily social, can I can speak of ‘my’ rituals, in the morning or other time, that are, as it were, personal and apply only to me as an individual. So here is the excerpt:
A ritual is a repeated, structured sequence of actions or behaviors that alters the internal or external state of an individual, group, or environment, regardless of conscious understanding, emotional context, or symbolic meaning. Traditionally associated with gestures, words, or revered objects, ….They may be prescribed by tradition, including religious practices, and are often characterized by formalism, traditionalism, rule-governance, and performance. / …
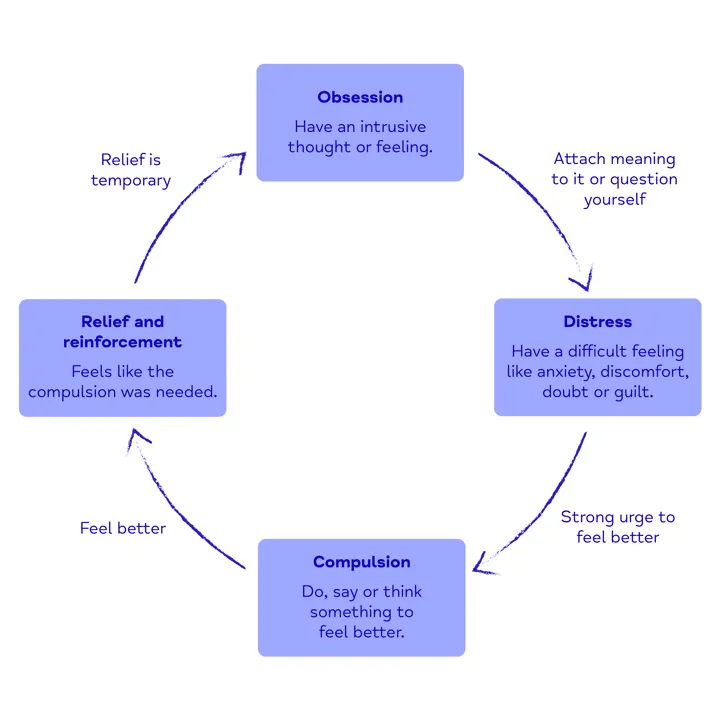
In psychology, the term ritual is sometimes used in a technical sense for a repetitive behavior systematically used by a person to neutralize or prevent anxiety; it can be a symptom of obsessive–compulsive disorder but obsessive-compulsive ritualistic behaviors are generally isolated activities.
Etymology: The English word ritual derives from the Latin ritualis, “that which pertains to rite (ritus)”. In Roman juridical and religious usage, ritus was the proven way (mos) of doing something, or “correct performance, custom”. The original concept of ritus may be related to the Sanskrit ṛtá (“visible order)” in Vedic religion, “the lawful and regular order of the normal, and therefore proper, natural and true structure of cosmic, worldly, human and ritual events”. The word “ritual” is first recorded in English in 1570, and came into use in the 1600s to mean “the prescribed order of performing religious services” or more particularly a book of these prescriptions.
There is a great deal of content in this excerpt that might help us. First, we should consider the origin of the ‘word’ in Ancient religions, though the idea of there being a “lawful and regular order of the normal, and therefore proper, natural and true structure of cosmic, worldly, human and ritual events”, applies equally to liturgical debates in the Elizabethan Reformed Church, where a difference in ritual behaviours could lead a cleric or particupant who was in ‘error’ to the stake to be burned alive.
The issue I want to derive first from this, however, is the role of prescription in ritual. Ritual is a thing that must be done because it is written that it should be done in ancient text/prescribed tradition (Vedas, the Talmud or Bible or Khoran) and oft, with varying degrees of exactness across traditions and cultures, must al;so be done in the exact order and performance values as was written there or in authorised exemplifications thereof.
This is vital in understanding the role of repetition and homostatic structural issues in tne meaning generalised by the word, again with minor variation. This is so in descriptions of their origin in religion and/or magicwherein ritual is understood as the engine of promoting a change in “the internal or external state of an individual, group, or environment, regardless of conscious understanding, emotional context, or symbolic meaning”. Such transitions in being relate often to ‘initiation’ into a religious group (as is sometimes thought in relation to the Eleusian mysteries) that changes both outward and /or inward behaviour and the meanings thereof, as in ‘baptism’ or in ‘coming of age rituals too.
The central issue in ritual here is that it is a dynamic procedure, producing change in a number of systems of being and meaning in the animal. However, a third issue can be extracted hete: the shifting meaning of the word between what we might call is social-psychologocal one to its role in individual psychology, irrespective of socialised meanings or cultural-textual or folklore authorised meanings.
I take issue here with the words in Wikipdia that say that ritual in modern psychology, which more strictly speaking should read psychiatry, are INDIVIDUAL because the context and categories addressed are medicalised socially-constructed mental ill-being concepts; namely of obsessive–compulsive disorder (OCD). The sentences I need to address are these that say that in psychology (we must read ‘psychiatry’ of course’:’
ritual is sometimes used in a technical sense for a repetitive behavior systematically used by a person to neutralize or prevent anxiety; it can be a symptom of obsessive–compulsive disorder but obsessive-compulsive ritualistic behaviors are generally isolated activities.
Such description stem from medical statistical generalisations (in texts in their current revised form such as the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) and the International Classification of Diseases (ICD-11), of tbe clustered phenomena or traits of a thing psychiatry has determined to be a disorder, often in a contested field. It is clai.ed that tbeze issues are determined from studying statically clusters of symptom entities, although the relationship to statistics in tne process is a tually quite a subjectively defined one.
My first objection to the Wikipedia statement is related to the shakiness of the objective claims made for the category, even in OCD, for the purpose of the diagnostic category is precisely first of all to fit by comparison an individual’s ‘delusions’ into that of generalised group definition of people with that ‘disorder’. Yet being fitted into such groups rarely yielded even the limited satisfaction to isolated individuals of being one of many; for early psychiatry bluntly thought of OCD as entirely delusional in its belief systems and militated against such people finding each other in a group, lest delusions be reinforced. It is claimed that psychiatry now is more nuanced but I doubt whether it has dropped the function of disabling delusion by challenge in OCD, or at the worst high does of anti-depressant or anti-psychotic medication.
However, it is important we remember this statistical definition of a virtual group when we read the point made in Wikipedia that OCD rituals ‘are generally isolated activities’. For they are claimed by psychiatry to be this in each individual because they match the same activities performed by a whole group, however isolated from each other. Often the behaviours are isolated or become more and more so because they are described in negative fashion, as ‘delusion’, ‘compulsion’ and as ‘abnormal’.
Recent versions of Cognitive Behavioural Therapy address these activities in ways tnat see them as not ‘symptoms’ but examples of ‘unusual behaviours’, that can be addressed in relation in terms of the meaning they have to the individual as a legitimate member of society rather than to their pathology generalised to the individual from medicalised group characteristics (see Richard P. Bentall’s pioneering work, Madness Explained, now old enough to be ignored .ore effectivel by mainstream psychiatry, if not in non-medicalsed psychology, than it was on its emergence).
That kind of work finds com.onality between supposed delusions and symbolic expression of beliefs about social behaviour. Moreover, these beliefs are often ones about the perceived difficulty of social transitions and change. Let’s take an example from my experience of work in primary care psychology. The case is old but I have disguised the characteristics (not just names) of the real person should they or their family ever read this. It concerns Miriam, a woman in her fifties who had presented to secondary hospital services for over ten years with expressed concern over her OCD symptoms, as they were described to her.
These involved elaborate rituals of hygiene and placement of things in space and time order that were causing disturbance to her, possibly as a reflection of family concern, and her son, with whom she lived in a remote village. These compulsions were causing despair but the GP found secondary mental health practitioners unable, or unwilling, to address them, insisting they were dangerous to treat, outside of prescribing medication that Miriam would not take.
The GP rather boldly referred her to me as a provider of sub-clinical psychological intervention, largely because he was as frustrated as the lady at the lack of help, even when distress had risen so high that the lady herself articulated suicidal thoughts and intentions, though not plans, nor a belief that she would proceed with the intentions given her need to protect, as she saw it, her son.
My work with Miriam was addressed not, as all thought a CBT educated primary care practitioner would to the compulsive behaviours themselves, addressing them with withdrawal scales aimed at reducing the behaviour (long the approach anyway of secondary services that were almost entirely behaviourist in orientation) but to the ‘obsessive, ideas. We addressed them as strong ideas that could not be put away easily or at all. Those ideas stemmed around the well-being of her daughter, who having left home for university a long time ago was rarely seen by her mother, having now a family of her own and living at great distance in another country.
Miriam disclosed that her self- hygiene behaviours always related to her fears for the safety of her daughter, an idea discouraged previously who stuck with the idea her obsession must be fear of infection. Shared with secondary services therefore, these unusually strong thoughts were treated as ‘obsessive delusions’. My approach was to socially normalize the fears symbolised in the link of ‘obsession’ to ‘compulsion’ and to avoid naming them as delusive. As we talked, it became clear that Miriam felt that her care for the daughter had lacked control, not least to emphasise the additional care she felt she needed over her brother.
She was guilty about this, reading her ‘loss’ of her daughter catastrophically, which is not as her son knew it to be. Her fear in relation to her activities was thatat, if she did not do them, and to the exact duration (hours) as believed she had neen told to be correct and precribed by people who knew better, her own mother, now deceased, for instance; her daughter would die. Under this pressure she would not relinguish her rituals either in nature, form or order. For this was the only thing she could control in order to make up for her feelings of failure in relation, it seems, both to her daughter and her own mother.
Now clearly Miriam was addressing her anxieties but tbe nature of tbe anxieties were based in social content, social ideas of family responsibility, care and control and the relation of these factors. The talk we had could not be thought of as straying into psychodynamic grounds but was based on biographical narrative sharing, at that time considered fit for Primary Care Health Workers appointed after their advent from the 2000 NHS plan.
The outcomes of this work, relatively short in duration, was a considerable reduction in tbe activities thought of as compulsive, but more importantly the massive reduction in measured (by questionnaire) distress and suicidal ideation. Miriam was considered well enough for the GP to implement the end of tne long non-working link with psychiatry and medication approaches, and our relationship too to come to a safe end, partly because one other effect was an increase in the quantity and quality of Miriam’s communication of her fears within both family and community, where she found analogies to her fears that had not been pathologised.
Now why do I recount all this? It is because those ‘obsessions’ were originated from morning (and evening) rituals that began to be attached to concerns about self-definitions and family responsibility, perhaps even guilt at favouring her son over her daughter in earlier life, what felt outside the ability of Miriam even to articulate or share without help. In this case she had been pathologised with a label – of a form of anxiety that led to medicalised interventions that led to less felt control over her life and a declining trend in her well-being over decades.

My issue here is that rituals (meal-time ones are even more interesting and equally capable of being used to understand eating ‘disorder’ in care and family settings) are also oft related to ideas of stasis set against change, prescribed control by family ideologies (no more substantial than other mental furniture but no less capable of taking the role of an obstruction to change) over psychosocial adaptation.
I find it, for reasons to be inferred from above, never to have rituals that are incapable of adaptation and consciously so, and never secret. But that makes them not rituals in my mind but adaptive cognitive scripts oe schemas, as easily rewritten (which because of thought automation and the role of tne cerebellum is not always that easy) as they are perceived as obstacles to necessary life-change.
With love
Steven xxxxxxx
