


Dedicated to Joanne
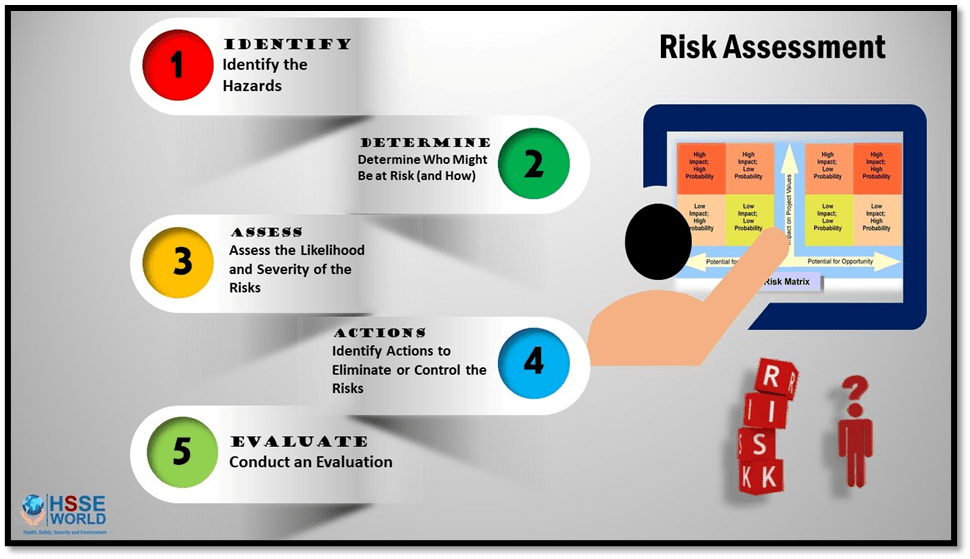
When I worked as a social worker I believed in and promoted in my own practice, and in the learners I worked with at Teesside University later as Subject Leader in Social Work, a concept called ‘positive risk-taking‘. It was a concept first popularised by Steve Morgan in an important article and devised for use initially in mental health services to refine the practice of risk assessment that included the person’s desire to live a life that, in order to be called life at all, involved some risks such as all of us take at all times. What it should have always meant was a collaborative dialogue between professionals in health and social care and people who use these services to support those lives with true care. What it increasingly meant was decided by cost-cutting strategies that justified institutions from positive intervention in lives in the name of enabling and a thinly defined thing the services called ’empowerment’. It meant withdrawing or denying service to encourage independence without discussion and just by citing the slogan that the institution believed in ‘positive risk-taking’.
When I used it, in a range of services, I used it as in this example (names changed):
Joe was a thirty year-old man with learning disability. Despite a life-time experience of stigma he found learning disability focused services a limitation in his life. He was aware of his need of peer support but wanted sometimes a holiday from learning-disability-labelled day-centres and group events. He longed for a holiday in which he used skills he had learned. Using this policy to stand against opposition in the department I worked in I organised such a holiday in a guest-house I scoped and negotiated with. I organised emergency support that I felt probably unnecessary with Joes’ participation (it involved signposting the provider of the guest accommodation to services local to them – also informed – and the offer of telephone support from myself should Joe need it). He used the latter prop once when he was subjected to the stigma of grotesque name-calling in a public place and became upset. As a result of the call, Joe was able to access emotional support (from the son of the guest-house owner, whom I knew and trusted) and went on to enjoy his holiday. Even when he missed his stop on the coach journey home (again organised by me), the driver was able to support him to take a short taxi-journey home.

This is not a picture of Joe but the smile is like his when he found the capacity allowed to him to work and play independently.
But a taste of what services became can be gauged from a study published this year of ‘positive risk-taking’ for people using occupational therapy services over 36 Local Authority areas (only 36 out of 106 [roughly 34%) chose to take part which tells its own story):
In all, 36 Local Authorities responded out of 106 contacted. A total of 21 documents were included for review. Substantial variability was found in terminology, definitions and risk grading between documents. The greatest consistency was found in how to implement a positive risk-taking intervention. Consistency was also found in the policy that documents cited. There was little reference to evidence to support intervention components. Overall, AGREE II quality scores were low and stakeholder involvement, specifically with regard to the views and preferences of service users, was largely absent. (1)
What concerns is that the area of consistency was highest where implementation was concerned, for that implementation amounted in the eyes of the people using the services to an unexplained denial of service in which the user of the service was not involved. That is a sorry tale of the absence of a true relationship between professionals and service users in which positive risk-taking was aimed at positives for the service alone: lower costs, lower stress of direct and indirect engagement.
This was not what Steve Morgan was talking about. When I first used the service in a Outreach Mental Health Team, I used it to work in case conferences to challenge professionals who resisted signposting and aiding service users to maximise their benefits (saying they would only abuse the money on drugs, without seeing positive capacity in the move for finding stimulation outside of drugs) or widening their experience safely in a collaborative manner – in their relationships (including sexual relationhips) for instance. The most abused were people with LGBTIQ+ relationships for whom any sexual or loving component was considered a no-no, especially in the case of trans services users with enduring mental health and learning difficulties. Consider the following:
Jane was a pre-operative trans woman in her twenties with a history of learning disability service and suicidality related to early sexual trauma caused by male parental abuse. She was allocated space in a huge tower block some 20 floorshigh in order that she had the flat directly underneath the office of the in-house carers. They claimed this was because of her suicide risk but the flat chosen had no window bar and could be used for suicide at easy convenience. This had been assessed as part of the balance of risks a Community Psychiatric Nurse (CPN) told me. The case team, before it included me, had lied to Jane about the delay in accessing transition surgery, well after living as a woman for the prescribed period, because her smoking was an risk. they even told me that as incoming social work team member. In the event on accompanying Jane to the GP on her request for another matter, for smoking cessation referral, We are told by the GP that the team were not telling the truth. The decision had been made to delay by the psychiatrist and lead nurse colluding with my predecessor. After being taken out of a case meeting and verbally abused by the psychiatrist for involving a trans advocate (the cis one colluded) , it was possible eventually to move on the transition plan safely by involvement of a team of gender dysphoria specialist (still dependent as we are on such diagnoses) and a move of house to a council house in a nearby estate. The health team at first said they would not visit her there because of the risk to them, the suicide risk at the high-rise having been forgotten. The last I knew Jane was doing well and living an independent life.
That services went to great lengths to deny Jane a life in the name of risk assessment was clear, Well after her well-being increased, I learned that services still took reports from the ‘home-care’ services from the high-rise office, who reported any sightings of Jane with me to them. In one, they informed my manager in the hope of finding collusion between an openly queer social worker and Jane. I could report back from my notes that the sighting involved merely me supporting Jane in equipping her new home with safety items.
Whether Jan ever benefitted from team interventions, I think it is no improvement to withdraw all support and call it positive risk-taking. People can only be empowered after the reasons for their original dis-empowerment are addressed. it was too easy to label all that ‘learned helplessness’, after Seligman’s bland researches (cruel experiments on dogs). People are empowered when all their resources are maximised – including psychological resources – not by neglect and leaving be in the belief that ALL interventions disempower. Addressing those inequalities always was what social work, that maligned discipline, was about. Social work is hard work – very hard work. it is about addressing inequalities of capital of all kind, including social and emotional capital until we start seeing that the word ‘capital’ is itself a misnomer. We are not economic assets, we are people. The role of socio-emotional and active intelligent resource optimisation should always be a part of positive risk-taking. It is the only way it works, if it ever works. All children, after all, regardless of any labels attached to them depend on our wisdom as adults in this area too. What we forget is that we easily INFANTILISE some adults.

Nevertheless my hopes are not high for the future. All instances above must now be from a long time ago, even before Steve Morgan. That study by Field et. al (at note (1) below) worries me a lot therefore.
With love and hope
Steve
______________________________________
(1) Leanne Field, Liana Nagy Tarnya Knaggs & Johnny Collett (2024) ‘Positive risk-taking within social care for adults with physical disabilities: A review of guidelines in practice in England’ in The British Journal of Occupational Therapy (First published online April 15, 2024) available at: https://journals.sagepub.com/doi/10.1177/03080226241246511
