Thursday, 9 Feb 2017, 20:39
Visible to anyone in the world- Edited by Steve Bamlett, Friday, 10 Feb 2017, 20:21
– Edited by Steve Bamlett, Thursday, 9 Feb 2017, 20:41
Review of:
Lewis, Marc (2015) The Biology of Desire: Why Addiction is not a Disease Melbourne & London, Scribe Publications
The value of this book can’t be under-estimated and should not be dismissed. Its target is the biomedical model of addiction – the disease model – and its success as a book for me was to further clarify the slipperiness of the term ‘biopsychosocial’ common to contemporary discussions of the aetiology, maintenance and the structuring of supportive interventions in addictions. My background in social work was an early attraction to the term ‘biopsychosocial’ as a means of bridging the divide in the debate between biomedical and psychosocial theories of addiction. However, in practice, this bridging tended to further bolster the biomedical model and relegate psychosocial intervention to a secondary role both in specialist intervention team structures and operations. Such teams often continued to be headed by a psychiatrist.
This for two reasons (although these reasons are solely the product of a retired practitioner’s reflections on past experience):
1. The ‘bio’ in the biopsychosocial was often regarded as the essential element on which to focus conceptually. This element is also conceived as owned therapeutically by biomedical sub-teams. The psychological and social domains were too also often treated as merely reflections of the biological on another ‘level of explanation’. That term derived from Fredrick Toates in the Open University.
2. Biomedical sub-teams increasingly colonised the psychosocial and, in doing so, gave to them a medical flavour, especially at the level of qualification to practice for practitioners and demonstration of that qualification in role and appearance – even dress (with priority given to nurse trained staff).
This feature is, of course, in part a product of institutionalised state health providers in the UK and less apparent therefore to Lewis in the USA, where the biopsychosocial is conceived as somewhat apart from the biomedical model. In his book, the ‘bio’ in biopsychosocial is a merely the name of organisation of a knowledge about embodied systems and systems that contain (as personality does) the body and is much easier to pit against a biomedical system that is essentially run for profit as it is in the USA.
I tried to draw this distinction in the following figure.
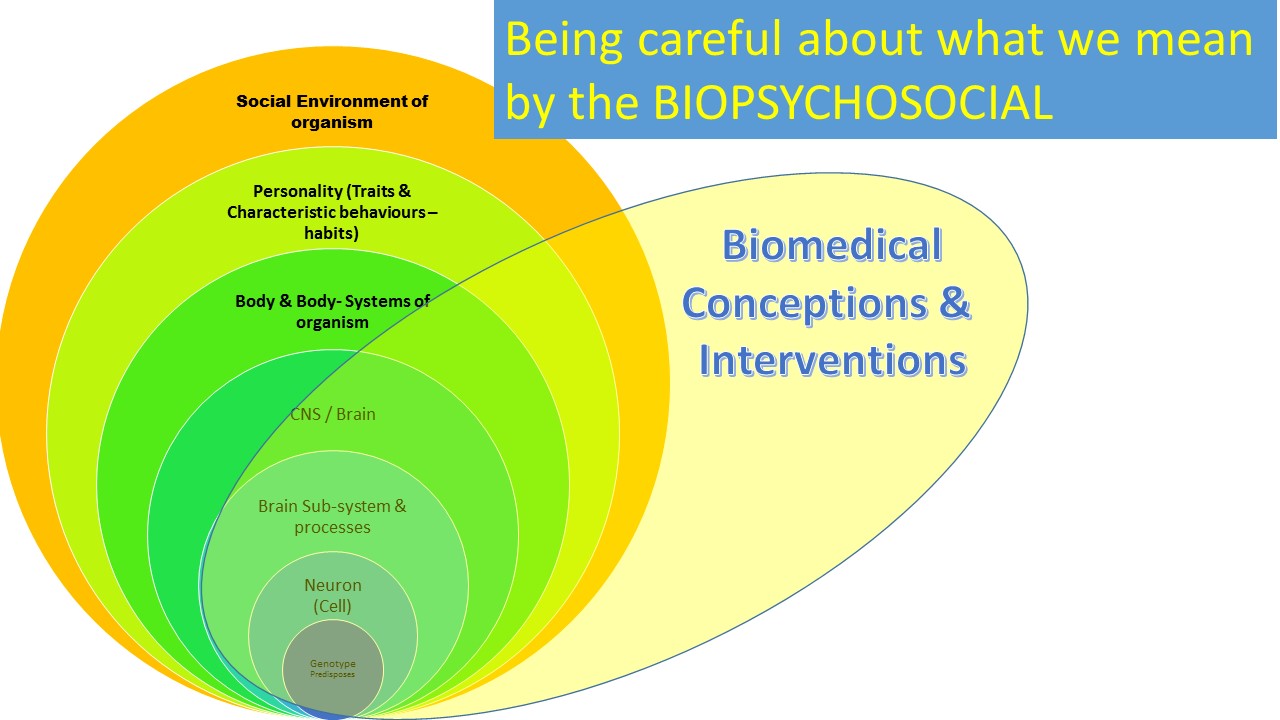
In the figure, the biomedical merely occupies the same terrain as a conceptual biopsychosocial model but it interprets that terrain differently – through the lens of qualified and exclusive practice by biomedical teams and ‘allied’ services.
Any realistic understanding of that figure will, of course, readily admit that there will be a trade between the biomedical and conceptual biopsychosocial but that both need to be kept distant from each other in our thinking, at least at the level of theory and intervention planning. As Lewis shows, some descriptions of neuronal activity can describe change in neurobiology and neuroanatomy in terms other than ‘disease’ and can make legitimate analogy between the features of socially validated and socially invalidated learning.
The processes involved in falling in, and out of, love and learning literature or neurobiology, all of which are about neurobiological change at some level, are also ‘normative’ learning processes that we do not describe in medical terms. To spell that out – all of these processes can be described at each level throughout the nested processes shown in our circular system map in the figure above but some, like ‘falling in love’ rarely are.
For Lewis, given free reign and dominance, the biomedical (even when it imports and colonises aspects of the psychosocial) retains interests that are solely its own – those of professional exclusiveness and top-down control of the person experiencing learning through addiction. His stories of the horrors of treatment centres ring very true to me from my working life (see p. 212). Of course, that is not to say I didn’t see islands of good personal practice.
One sign of the difference in the way the biopsychosocial is conceived in Lewis is the Birmingham Reach Out Recovery (p. 214) intervention in which a large part of the intervention was fuelled by consulting groups of former addicts who worked with each other to socialise and increase access to support. Often that support appears little less than the provision of venues, such as ‘recovery-friendly shops’, for the ‘addict’ to build on and generate new story from their old stories, stories which appear to have got stuck in ‘now-appeal’ as he calls ‘addiction’.
That this is more truly biopsychosocial, Lewis argues, is seen in the deficiencies of time and professional personnel controlled CBT and even mindfulness interventions that measure input and output but do not generate motivation or change (in themselves). The stress is on narrative (I can see the biomedical teams now developing training for nurses in ‘narrative therapy’ – indeed it has been happening some time) but not narrative aimed at ‘therapy’ as such but in generating motivated movement in the stalled neuroplasticity in the brain of the addict (locked into what Lewis call ‘now-appeal’).
So if desire cannot be turned off or seduced away from addictive goals, then it has to be fastened to goals incompatible with addiction – goals such as freedom from suffering, achievement of life projects, access to loving relationships, and the sense of coherence and self-love that can come with abstinence. And if those goals cannot be envisioned, because of a static pre-occupation with the present, then self-narrative and desire need to be packaged together – self-narrative to shift perspective to long-range goals, desire to power the pursuit of these goals.
Stories don’t work without emotional themes. They would be impossible to follow. ….
This (from a neuro-scientist) is now conceivable because neuroscience, unlike the sterile discipline of cognitive psychology, has freed itself from a merely cognitive and merely behavioural interest – its interest in those brain processes called emotion and drive would have shocked Skinner, Pavlov, and Beck. Now no-one dare write about psychology without recognising ‘Descartes’ Error’ (Antonio Damasio).
So this book genuinely revels in all its centre parts on biographical (and some autobiographical), stories of addiction that are a long way from the mechanical nature of the Jellinek curve. Its bookend chapters are helpful though with definitions of brain anatomy and processes that can be understood by anyone – and while this book can replace no textbook accounts for a learner in higher education, it can make their limitations and gaps clear to both pure scientists and practitioners: pure science, that is, which is not still married merely to positivism. Look for instance at the genius of the everyday science explanation of the anatomy and function of the Orbito-Frontal Cortex (p. 82). If you are a beginning learner (or even if you began a while ago) you can learn a lot from that.
I love this book.
Steve

I was pretty pleased to discover this site. I
wanted to thank you for your time for this wonderful read!!
I definitely enjoyed every part of it and I have you book marked to see new things on your
web site.
LikeLike